In the ever-changing pharmaceutical landscape, a compelling medical narrative is key to shape persuasive stories for stakeholders, guiding internal decisions and engaging field professionals. This white paper defines the essential elements to craft impactful medical narratives and explores how these can be adapted to diverse audiences and evolving industry landscapes.
In this white paper, you will:
Understand the crucial role of medical narratives in communicating a product’s value proposition to healthcare professionals, patients, regulatory bodies and payers
Discover the macro trends, healthcare ecosystem complexities and product-specific details that shape effective medical narratives at different levels
Learn the foundational elements to craft a compelling medical narrative, from articulating scientific and clinical properties to understanding audience needs
Understand how to integrate past, present and future perspectives into your narrative and access our framework to guide your journey
Don’t miss out – download your free copy of this white paper by completing the form.
Though helping pharma brands succeed is what drives our business, we are acutely aware that our real mission is to help pharma deliver better outcomes for patients. In fulfilling our roles, we have the privilege of speaking to and connecting with patients across the globe, understanding their healthcare challenges and relaying them to empower brands to make a difference.
Over the years, we have spoken to countless oncologists and patients who have generously opened up about their experiences with cancer. As a result, we have gathered rich and nuanced insights into the real-world impact of cancer and the different ways in which it can affect people’s lives.
To mark International Women’s Day, we wanted to shed light on some of the social and emotional issues that have an impact on outcomes for women with cancer, focusing on detection and diagnosis. We know that early diagnosis is crucial to improved outcomes, but we do not always consider the gendered nuances at play.
Such nuances are evident in the prevalent late-stage diagnosis of women with cancer. It is no secret that women often deprioritize their own health as the primary caregiver in their family unit. As our Life Sciences Director Michaela Scheiner puts it: “A woman has so many roles to play […] she is the daughter, the wife, the homemaker, the worker. At some point, her health just becomes another hat to wear.” This is more than a cultural cliché: It can have a tangible impact on the prognosis for women with cancer by delaying how long they wait to present their symptoms to a doctor. . For example, a global 2022 study found that the prevalence of late-stage presentation among patients with cervical cancer stood at 60.66% .[1]
We have found that for women of ethnic minorities living in the US and EU, these sentiments are stronger. As part of a wider study of cancer inequalities conducted in 2023, we spoke to several South Asian women living with various tumor types in the UK. The notion that a woman’s needs are subsidiary to those of her husband or children is reinforced by a pervading cultural belief that it is indulgent or selfish to become preoccupied with one’s health. This is compounded by lower levels of education and limited awareness of different cancer symptoms, exacerbated by language barriers that hinder mainstream campaigns on breast checks, cervical screenings and other preventive health measures from reaching these demographics. As Nila Sanyal, our Commercial Consulting Director who conducted these interviews, reflects: “All of these factors provided a fertile ground for festering misconceptions and myths, all of which contributed to the woman not accessing medical professionals in a timely manner.’’
Women face further challenges once they present with cancer symptoms. ‘Healthcare gaslighting’ is a phenomenon in which women are less likely than men to be taken seriously by medical professionals. I vividly remember a male neurologist telling me during a market research interview about chronic pain that women “don’t tolerate pain as well as men” and therefore “complain more”. I was dumbfounded, and these attitudes can have dire consequences within oncology. The Every Woman Study of patients living with ovarian cancer in Canada found that 30% of patients who waited more than three months for a diagnosis felt like their healthcare provider had ‘brushed off’ their concerns about their symptoms.[2] It complicates matters that common symptoms of gynecological cancers, such as irregular bleeding or abdominal discomfort, are often considered normal aspects of ‘being a woman’.
Again, we have seen that women from ethnic minorities face additional challenges when presenting with cancer symptom. Cultural factors can cause feelings of unease and embarrassment when it comes to discussing intimate areas, while language barriers can prevent open communication about symptoms. We have also heard that women of ethnic minorities feel like healthcare professionals are less likely to take them seriously due to racial prejudice, and they might have to present multiple times before additional investigations are undertaken or appropriate referrals are made. The statistics speak for themselves: In a recent study published in the British Medical Journal, it was found that Caribbean and African women are more than twice as likely to be diagnosed with late-stage uterine cancer than white British women, 85% more likely to receive a late-stage ovarian cancer diagnosis and 71% more likely to receive a late-stage breast cancer diagnosis.[3]
There are many avenues for pharma to explore to make a tangible difference in reducing the overall cancer burden for female patients. The fundamental building blocks are centered on encouraging women to prioritize their health, empowering them with information so that they can be vigilant of the various signs and symptoms of different cancers. This means investing in grassroots programs in schools to teach girls from a young age that their health is not a ‘taboo’ subject to be avoided but rather a priority. Pharma must continue to partner with government bodies, PAGs and NGOs to ensure that they are directly providing ‘on-the-ground’ support for screening programs both in the West and in underdeveloped nations – providing the infrastructure and publicity to encourage routine checkups that can drive early detection. Moreover, R&D that is focused on developing more accurate and timely diagnostic tools will help build faith in the screening process and encourage women to proactively take charge of their own cancer risk.
There is no blanket approach to improving the detection and diagnosis of cancer in women. Any strategy must consider the additional challenges faced by women of diverse cultural backgrounds, with tailored messaging anchored in relevant cultural codes disseminated via niche, non-mainstream channels.
Leveraging a feminist perspective in the battle against cancer will reap benefits for healthcare systems and communities, transcending boundaries and elevating overall population health.
Special thanks to Sukanya Saha, Director; Yasemin Yildiz, Director; Michaela Scheiner, Director; Nila Sanyal, Director; Olga Fidalgo Gonzalez, Associate Vice President; Deana Scott, Director; Helena Cannon, Director; and Emma Brooks, Consultant, for their contributions to this piece, in addition to the countless women who have given me their time during my four years at Prescient to share their experiences with cancer.
Disclaimer: We recognize that individuals affected by cervical, ovarian and breast cancer might not exclusively identify as women. We acknowledge the diverse spectrum of gender identities and emphasize that separate health issues exist for men, trans individuals and others. Our intention is to shed light on the challenges faced by individuals traditionally associated with women’s health issues while respecting and acknowledging the broader context of gender diversity within the realm of cancer awareness.
With the end of JPM 2024, we reflect on the state of the pharma deal universe and look to a future of intense competition where only flawless execution will deliver success. consensus on the annual event, which traditionally kicks off and sets the tone for the year, seems to be moderately positive. We look beyond the headlines to anticipate future direction, with the context provided by the past.
Position of JPM in pharma M&A:
After a couple of quiet years, JPM is back with a steady flow of deal announcements but this followed a significant uptick in the deal flow in Q4 2023. A billion-dollar buyout announced just days before the event, demonstrates that deals are not waiting for JPM announcements anymore. Nonetheless, JPM is set remain a key event and serve as the year’s starting gun in large segments of our industry. Nonetheless, it is clear that companies are not waiting for JPM to announce their deals anymore,.
Deal analyses:
As inrecent years,sub-$5B bolt-on deals have been the majority
Oncology was prominently featured again, with the biggest deal by value being the $2B acquisition of Ambrx by J&J
Similar to the Merck acquisition of Harpoon, such bolt-on deals provide access to buzzy platforms and, critically, center around assets with promising clinical data that are complementary to the buyer’s portfolio
In December 2023, there were some large bets in neuroscience (Karuna at $14B and Cerevel at $8.7B). Though the interest in this therapeutic area remains strong, at JPM, there was more talk than action (MedTech acquirer Boston Scientific’s $3.4B deal on neuromodulation was the big news)
Many are saying that, as different sides of the same coin, Immunology is the new oncology”. Accordingly, many of the learnings from immuno-oncology are being translated into immunology. The influx of CAR-T studies in SLE, driven by strong early data, is notable, as is the opportunistic expansion of Regeneron’s linvoseltamab program, in combination with dupilumab, into food allergy
The utility and eventual impact of AI continues to divide opinions, but deals continue to flow in early stages, with both Isomorphic and Nvidia making headlines leading up to the event
Bottom line – Megamergers are a thing of the past, at least for now. The FTC’s attention, IRA’s implications on launch control and the cost of debt may all be weighing on this, but Pfizer-Seagen demonstrates the potential for big acquisitions when companies are the right fit. Pharma search and evaluation scouts continue to be highly active with asset-centric remit; at JPM 2024, Takeda described how “almost every biopharmaceutical company” was evaluating Nimbus at the time of its acquisition in 2022, even though the company had executed a down-round a few months earlier. Clinical data remain key enablers of deal-making, but valuations rely much more on circumstance, which is perhaps why the Novartis-Cytokinetics discussions (big rumor at JPM) never reached a transaction. The biotech downturn has resulted in a distillation in target companies, even as trend for pharma to fast follow peers into validated drug targets and markets continues. .
What does this mean for our biopharma partners?
The cyclical nature of our industry allows us to predict the future with some confidence. We see patent cliffs having a broad impact across Big Pharma, which, with >$1T in firepower to deploy, must now take on a pipeline restocking exercise. Healthcare VCs have raised over $90B over the last four years to drive innovation, and there are signs that the IPO market is opening up again. We anticipate that there will be growing competition and increasing valuations around mid-stage validated assets, especially pre-launch. With all pharma companies experiencing similar macroeconomic pressures, BD strategies are likely to be differentiated on portfolio management and R&D development.
Increased competitive intensity, decreased regulatory flexibility and increasing reimbursement challenges all mean that it is more important than ever to get BD, development, launch and lifecycle management right the first time. The winners will be those with the foresight to provide new drugs that are positively differentiated by data and customer perception. Contact Prescient today to see how our view of the dynamic present can inform your future, combining hindsight, insight and foresight..
Prostate cancer ranks as the second leading cause of cancer-related deaths in the US, with approximately 34,700 fatalities due to this disease in 2023. Further, this is also the most commonly diagnosed cancer among men, with a predicted incidence of 288,300 cases in the same year1. Prostate cancer usually begins as a slow growing, immunologically cold, solid tumor. While, in the majority of cases, the cancer initially responds well to androgen-deprivation therapy (ADT), as it progresses, it has the potential to metastasize and develop resistance, leading to metastatic castration-resistant prostate cancer (mCRPC). mCRPC is characterized by clinical, radiographic or biochemical progression despite treatment with ADT. In the US, there were approximately 98,000 cases of mCRPC in 2022 and the prevalence is expected to rise approximately 10% over the next 5 years2, which presents a tremendous challenge for patients and healthcare providers (HCPs). Despite the approval of novel compounds, mCRPC still yields poor outcomes, being associated with a median OS of approximately 1-3 years, varying on the location of metastasis3,4.
2. Evolution of the treatment landscape:
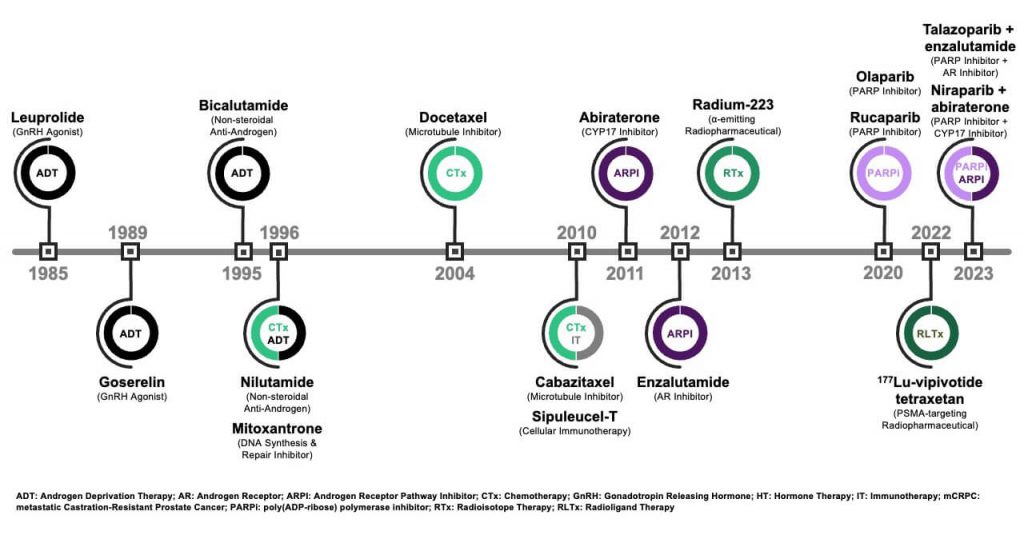
The treatment options for mCRPC have historically been limited, primarily featuring chemotherapy and palliative care. The first breakthrough in mCRPC treatment occurred in 2004 when docetaxel chemotherapy was approved by the FDA, driven by its OS benefit5. Docetaxel is effective as a first-line (1L) option for rapidly progressing mCRPC and in cases with visceral metastases. This approval marked a shift in the mCRPC treatment paradigm from palliative care to therapeutic care that prolongs survival. Following docetaxel’s approval, another taxane-based treatment, cabazitaxel, was approved in 2010. Over the subsequent three years, the treatment paradigm expanded beyond chemotherapy, offering more options for patients and prescribers, as shown in Figure 1. Androgen receptor pathway inhibitors (ARPI), also known as novel hormonal therapy, and additional options for specific subpopulations, such as sipuleucel-T and Radium-223, were introduced during this period. The last few years saw a third wave of innovation, with the approval of poly(ADP-ribose) polymerase inhibitors (PARPi) and PSMA-targeting radiopharmaceuticals.
Figure 1. Approval Milestones for Advanced Prostate Cancer
Current 1L options6 for mCRPC include ADT in combination with an ARPI, such as abiraterone, a CYP17 inhibitor that interferes with intra-tumoral androgen synthesis, or enzalutamide, an androgen receptor (AR) antagonist. Both agents have comparable efficacy and are prescribed based on AE tolerability, physician preference and payer-specific considerations7,8. Docetaxel also remains as a 1L option. The PARPi olaparib9 and niraparib10 can be used in combination with abiraterone for patients with breast cancer gene (BRCA) mutations, while talazoparib in combination with enzalutamide is also an option for patients with mutations in other homologous recombination repair (HRR) genes11.
The treatment options in second-line (2L) focus on changing mechanisms of action (MoA) from 1L, depending on the initial therapy (e.g., ARPI is followed by chemotherapy). For patients who have been previously treated with both ARPI and taxane-based chemotherapy, lutetium (177Lu)-vipivotide tetraxetan, a prostate-specific membrane antigen (PSMA)-targeting radioligand agent, can be used as a treatment for PSMA-positive mCRPC12. Further options that have demonstrated notable OS benefits include sipuleucel-T, an autologous vaccine immunotherapy for asymptomatic/minimally symptomatic mCRPC13, and radium-223, an α-emitting radioisotope for mCRPC cases with bone metastases.
3. Recent mCRPC pipeline updates:
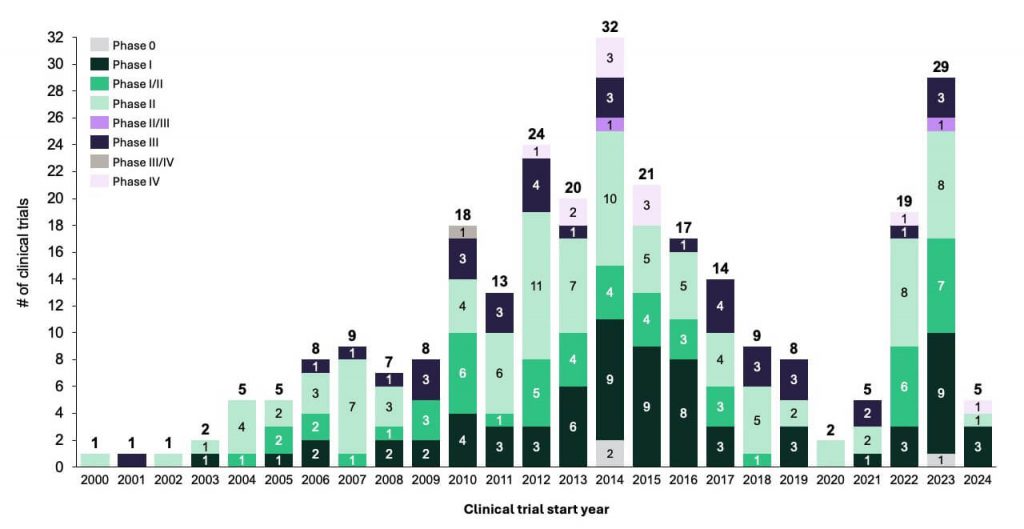
While a curative agent has not been developed, there is an ongoing effort to develop new life-extending treatments for mCRPC, stemming from the significant unmet needs in this area. Recent successes and the identification of options with novel MoA have led to a strong increase in trial activity (Figure 2). The primary focus is on pursuing novel treatments that minimize cross-resistance, improve survival outcomes and optimize therapy sequencing to maximize patient benefits. In the following sections, we will explore the growing pipeline of agents, examining their MoA, ongoing clinical trials and the potential impact on the evolving landscape of mCRPC.
Figure 2. Clinical Trials in mCRPC
a) Novel radiopharmaceuticals changing the treatment paradigm for mCRPC
Radioligand therapy is becoming a crucial element for prostate cancer treatment. In March 2022, the FDA approved 177Lu-vipivotide tetraxetan (Pluvicto™) as a 2L treatment for PSMA-positive mCRPC, following treatment with ARPIs and taxane. This approval was based on the favorable results from the Phase III VISION trial (NCT03511664) comparing 177Lu-vipivotide tetraxetan to the best standard of care (BSoC), which showed that the former led to improved radiographic progression-free survival (rPFS) and OS than the latter. Several clinical trials are underway to assess this asset’s efficacy in earlier lines of therapy. The interim results from the Phase III PSMAfore trial (NCT04689828), conducted in the earlier pre-taxane mCRPC setting, were presented at ESMO 202314. The results showed that 177Lu-vipivotide tetraxetan achieved the rPFS primary endpoint (12.02 months with 177Lu-vipivotide tetraxetan compared to 5.59 months in the ARPI control arm). Furthermore, this asset has demonstrated a remarkable ten-fold increase in complete response rate (21.2% vs. 2.7%) vs. the comparator arm. Further data from PSMAfore, including OS, will guide the FDA filing planned for 2024. Expansion plans into earlier lines are underway, contingent on the data readout from the PSMAddition trial (NCT04720157).
A similar agent, 177Lu-PNT2002, recently received Fast Track Designation from the FDA15. This agent is being investigated in a Phase III trial (NCT04647526) as treatment for PSMA-positive mCRPC patients that progressed after ARPI therapy and refuse or are ineligible for chemotherapy. The trial readout is anticipated in 2024. Additionally, 177Lu-PSMA-I&T, another radioligand, is under investigation both as a standalone treatment (NCT05204927) and in combination with 223Ra (NCT05383079) for mCRPC16. The wave of momentum for radioligand therapy in prostate cancer seems poised to persist into 2024.
b) Emerging MoA in mCRPC
Ongoing research is exploring the viability of alternative treatment modalities for mCRPC. These include kinase inhibitors (e.g., abemaciclib and capivasertib), bromodomain extra-terminal (BET) inhibitors (e.g., ZEN-3694) and AR-degrading agents (e.g., bavdegalutamide). Therapies seeking to increase the immunogenicity of tumors, such as bispecific antibodies and chimeric antigen receptor T-cell therapies (CAR-T), are also being actively explored.
Proteolysis-targeting chimera (PROTAC) AR degraders, such as the 1st generation bavdegalutamide, recently garnered attention as a potential option for a subset of mCRPC patients who carry AR ligand binding domain (LBD) mutations, who constitute approximately 10-20% of all mCRPC patients. Patients with these mutations often face a poor prognosis, as the frequency of the mutations increases with ARPI treatment and is thought to be linked to treatment resistance17. The Phase I/II trial (NCT03888612) evaluating bavdegalutamide acted as a proof-of-concept for the notable clinical efficacy of this asset in patients with AR LBD mutations; new data shared at ESMO 2023 showed a median rPFS of 8.2 months (95% CI: 3.8–not reached) with this drug in AR LBD mutant patients18. The 2nd generation AR degrader ARV-766, however, exhibited higher efficacy compared to its predecessor. PSA50 was achieved in 41% of all LBD patients receiving ARV-766 in a Phase I/II trial (NCT05067140), according to the interim results. Furthermore, ARV-766 exhibited a better safety and tolerability profile. These results, combined with ARV-766’s estimated potential to benefit a larger group of patients with mCRPC and mCSPC, led to it being prioritized for Phase III progression in mCRPC and mCSPC19.
Other notable mentions include antibody-drug conjugates (ADC) in development for mCRPC. HS-20093, a fully humanized IgG1 that selectively binds to B7-H3, a target that is abundantly expressed on solid tumor cells, had an acceptable safety profile and showed promising antitumor activity, as demonstrated by the partial response to therapy observed in the Phase I ARTEMIS-001 trial (NCT05276609). This led the asset to advance into a Phase II clinical trial (NCT05276609).
c) Novel combinations
The exploration of novel combinations of agents with complementary MoAs has been another promising strategy for the treatment of mCRPC. One notable combination to watch for in 2024 is cabozantinib, a tyrosine kinase inhibitor (TKI), plus atezolizumab, an immune checkpoint inhibitor. This combination has already achieved the primary endpoint of PFS in the pivotal Phase III CONTACT-02 trial (NCT04446117)20. Additionally, a positive trend for OS improvement was observed with the cabozantinib and atezolizumab combination compared to a second combination with ARPIs (e.g., abiraterone plus prednisone or enzalutamide) in patients with previously treated mCRPC. Definitive conclusions, however, cannot be drawn until OS data maturity is reached in H2 2024.
Additional studies evaluating combinations to monitor include a variety of trials exploring radioligand combinations21. Noteworthy among them is the Phase II EVOLUTION trial (NCT05150236), investigating the safety and efficacy of 177Lu-PSMA-617 combined with ipilimumab and nivolumab, immune checkpoint inhibitors, with an estimated completion in H2 2024. Additionally, the Phase III ProsTACT trial (NCT04876651) compares the combination of 177Lu-rosopatamab tetraxetan and an HCP’s preferred BSoC, such as taxane or ARPI, against BSoC monotherapy. ProsTACT, initiated in November 2023, is projected to conclude in Q4 202722.
4. Utility of genomic profiling in treatment selection
Understanding the genomics of prostate cancer is crucial to tailor effective treatment strategies, particularly for mCRPC patients. Genomic testing, encompassing germline and somatic assessments, plays a pivotal role. Additionally, RB, PTEN or p53 mutations may not only impact treatment decisions but also carry a substantial prognostic and predictive value23. The recent approvals of PARPi highlight the need to routinely identify mutated signaling pathways, as DNA repair mutations are present in approximately 23% of mCRPC cases.
There has been a surge in routine mCRPC genetic testing and a consensus in recommending integrating cancer genetics into the care plan. There are several implementational challenges, such as the rising demand for genetic counseling and testing, combined with existing accessibility barriers (e.g., geographic constraints on in-person services), which have created bottlenecks in testing. While considerable progress has been made, the routine application of genomics in mCRPC globally is still evolving24. Ongoing trials aim to strengthen the routine application of genetic testing as a standard for patients25, while research for treatments targeting other pathways, as described above, will further increase the need for testing over the coming years.
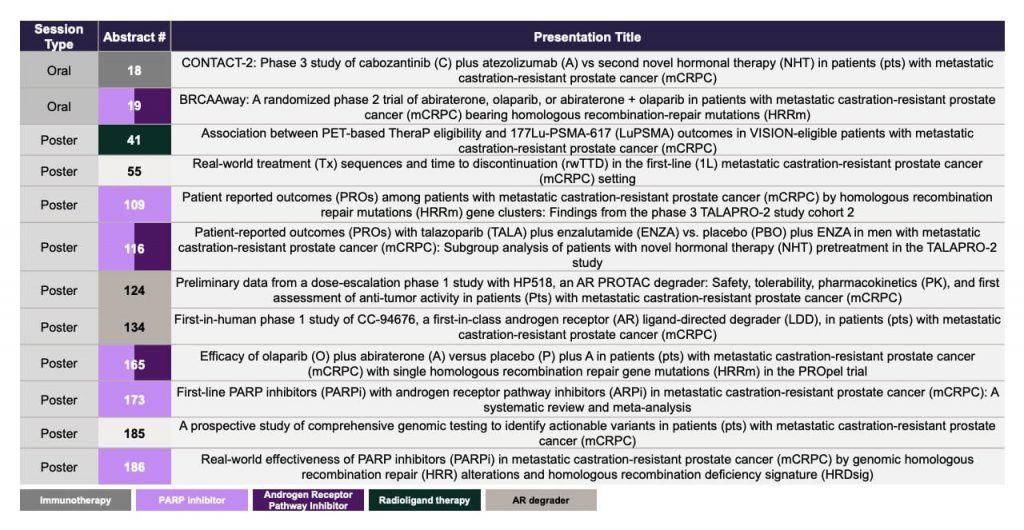
5. Outlook
The evolving landscape of mCRPC treatment, which is driven by ongoing research and innovative approaches, offers the potential for a deeper understanding of the molecular intricacies of advanced prostate cancer and novel treatment options for patients. The increased research activity can be expected to produce a wealth of new data over the coming years. Updates on novel treatment options, treatment sequencing, biomarkers and genetic testing will be presented at the upcoming American Society of Clinical Oncology Genitourinary Cancers Symposium (ASCO GU) on January 25-27 202426, with a selection of noteworthy abstracts highlighted in Figure 3. The symposium is positioned to enhance our understanding of prostate cancer and provide an outlook into the future of the treatment options for mCRPC.